Featured Answer: Dentures vs implants — which is right for you?
In the choice of implants vs dentures, implants anchor your prosthesis, reducing slipping and improving chewing. They help preserve bone and protect facial structure—delivering better function and confidence than adhesive-dependent dentures. Traditional dentures restore only 20 to 25 percent of natural chewing efficiency. Implant overdentures restore 60 to 80 percent. Fixed full-arch bridges restore up to 90 percent. That difference changes what you eat, how you speak, and how your jaw ages over the next 20 years.
If you wear traditional dentures and find yourself dealing with slipping, sore spots, or a shrinking jawline, you are not alone. The American College of Prosthodontists (ACP) estimates that 36 million Americans are completely edentulous (missing all teeth), and roughly 120 million are missing at least one tooth. Many patients across Marlborough, MA and the MetroWest region visit Innova Smiles seeking a more stable, comfortable alternative. Dr. Ambereen Fatima helps patients understand the full spectrum of options, from traditional dentures to implant-supported solutions, so they can make an informed decision based on anatomy, lifestyle, and budget—not a sales pitch.
Problems with Traditional Dentures
Traditional dentures rest on the gum ridge and rely on suction or adhesive for retention. They have been the standard solution for complete tooth loss for centuries, and modern dentures are better made than ever. But even the best conventional denture has fundamental limitations that no amount of improved materials can fully overcome.
Movement and Sore Spots
Lower dentures are notoriously unstable because the lower jaw ridge is narrower and the tongue constantly displaces the prosthesis. Upper dentures fare better because the palate provides a larger surface for suction, but even upper dentures loosen over time as the ridge shrinks. The friction from a poorly fitting denture creates sore spots, ulcers, and chronic irritation of the oral mucosa. A study in the Journal of Prosthodontic Research (2019) found that 65 percent of denture wearers reported at least one episode of significant soreness per month.
Adhesives and Dietary Limits
Denture adhesives are a $300 million per year industry in the United States—a testament to how common denture instability really is. Even with adhesives, most denture wearers avoid hard, crunchy, or sticky foods. Apples, corn on the cob, steak, raw vegetables, nuts, and caramel become off-limits. A 2018 study in the Journal of Dental Research found that complete denture wearers consumed 40 percent fewer fruits and vegetables than dentate (teeth-bearing) individuals, which has real nutritional consequences—particularly for older adults who already face elevated risks of malnutrition and vitamin deficiency.
Ongoing Bone Loss and Changing Fit
This is the most serious long-term consequence of conventional dentures. When teeth are extracted, the jawbone no longer receives the mechanical stimulation from chewing forces transmitted through tooth roots. Without that stimulation, the body resorbs the bone. According to the ACP, denture wearers lose an average of 0.5 to 1.0 mm of alveolar ridge height per year. Over 10 years, that is 5 to 10 mm of bone loss—enough to make the original denture completely unwearable and to alter facial appearance dramatically.
The clinical term for severe bone loss in the jaw is "residual ridge resorption," and it follows a predictable pattern. In the first year after extraction, patients lose approximately 25 percent of the ridge width. By year five, the vertical height has decreased noticeably. By year 10 to 15, some patients have lost so much bone that even relining the denture cannot restore stability. This is the point where many patients from Northborough, Southborough, and surrounding communities come to our office looking for alternatives.
The Bone Loss Timeline Without Implants
| Time After Extraction | Average Bone Loss | Clinical Impact |
|---|---|---|
| 0–6 months | 25% ridge width | Denture fits well initially |
| 1–2 years | 40–60% ridge width | First relining needed |
| 3–5 years | 2–4 mm vertical height | Denture loosens noticeably, sore spots increase |
| 5–10 years | 5–8 mm vertical height | Second denture fabrication often needed |
| 10–20 years | 8–15+ mm vertical height | Severe ridge atrophy, facial collapse, difficulty wearing any denture |
This timeline is not hypothetical. It is documented in longitudinal studies published in the Journal of Prosthetic Dentistry and the Clinical Oral Implants Research journal. The facial changes—sunken cheeks, collapsed lower face, protruding chin, thinned lips—are what many people associate with "looking old." Much of that appearance change is actually bone loss from missing teeth, not aging itself.
Implant-Supported Solutions
Dental implants address the fundamental problem of conventional dentures by replacing the tooth root. A titanium implant post integrates with the jawbone through a process called osseointegration, creating a permanent anchor that transmits chewing forces into the bone—just like a natural root. This stimulation preserves bone density and prevents the resorption cascade described above.
Two main categories of implant-supported prostheses exist:
Implant Overdentures (Snap-On Dentures)
An overdenture snaps onto two to four implants using attachment systems such as locators or bar clips. The denture is still removable for cleaning, but it stays firmly in place during eating and speaking. This option is often more affordable than a fixed bridge and dramatically improves stability compared to a conventional denture.
The concept is straightforward: implants provide the retention that adhesive and suction cannot. The overdenture clicks into place over the implant attachments and does not move during function. You remove it at night for cleaning, just like a conventional denture, but during the day it is rock-solid.
How many implants are needed? For the lower jaw, as few as two implants can support an overdenture—this is actually the minimum standard of care recommended by the McGill Consensus Statement (2002), which stated that a two-implant overdenture should be the first-choice treatment for the edentulous lower jaw. For the upper jaw, four implants are typically recommended because the upper bone is less dense and needs more support points.
Attachment types:
- Locator attachments: Small, low-profile nylon inserts that snap onto the implant abutments. They are the most common system because they are easy to maintain (the nylon inserts are replaced during routine dental visits when they wear out) and tolerant of slight misalignment between implants.
- Bar-clip systems: A metal bar connects the implants, and the denture clips onto the bar. This provides more retention than individual locators and better splints the implants together for load distribution. The downside is slightly more complex fabrication and higher cost.
- Ball attachments: Spherical abutments that snap into corresponding sockets in the denture. Less common today than locators but still used in some cases.
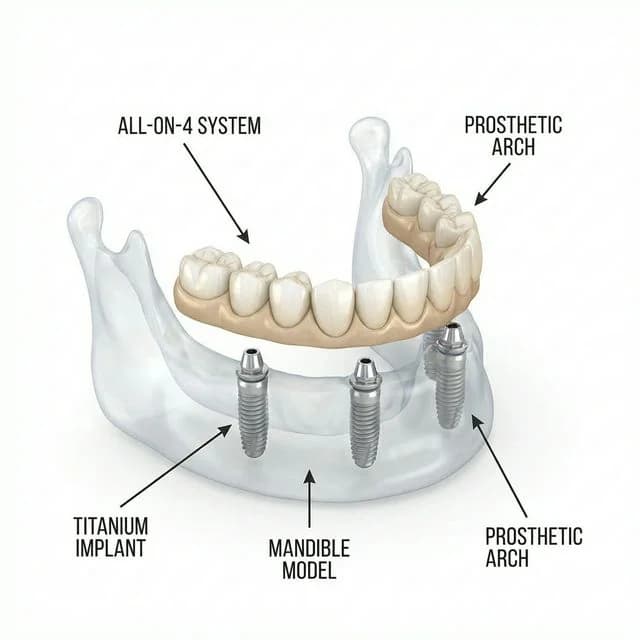
Fixed Full-Arch Bridges (All-on-4 / All-on-X)
A fixed full-arch bridge is permanently attached to four or more implants and can only be removed by your dentist. Research published in the International Journal of Oral & Maxillofacial Implants shows that fixed full-arch prostheses supported by four or more implants achieve long-term success rates above 95 percent at 10 years. It feels and functions much more like natural teeth, eliminating the need for adhesives entirely. Patients who choose this option often describe it as life-changing.
The All-on-4 concept, developed by Dr. Paulo Malo in Lisbon, uses four strategically angled implants to maximize bone contact and avoid anatomical structures like the maxillary sinus and the inferior alveolar nerve. The posterior implants are tilted at approximately 30 to 45 degrees, which allows them to engage longer sections of available bone without requiring bone grafting in many cases. This was a breakthrough because it made fixed full-arch treatment accessible to patients who previously would have needed extensive grafting before implant placement.
The All-on-4 treatment timeline:
- Day 1: Extractions (if needed), implant placement, and delivery of a temporary fixed prosthesis. You leave the office with teeth.
- Months 1–4: Healing phase. The implants integrate with the bone. You wear the temporary prosthesis, which is functional but not the final restoration.
- Month 4–6: Final impressions are taken, and the permanent prosthesis is fabricated by our lab partner.
- Month 5–7: The permanent fixed bridge is delivered and torqued onto the implants. This is your definitive restoration—zirconia or acrylic hybrid, depending on your case.
Dental Implants vs Dentures: Side-by-Side Comparison
| Factor | Traditional Dentures | Implant Overdentures | Fixed Full-Arch (All-on-4) |
|---|---|---|---|
| Stability | Low to moderate | High | Highest |
| Bone preservation | None—bone loss continues | Moderate—slows resorption at implant sites | Best—stimulates bone across the arch |
| Chewing efficiency | 20–25% of natural | 60–80% of natural | up to 90% of natural |
| Bite force | 25–35 lbs | 75–150 lbs | 150–200+ lbs (near natural) |
| Adhesive required | Often | No | No |
| Removable | Yes | Yes (for cleaning) | No (only by dentist) |
| Palate coverage (upper) | Full palate covered | Partial or no palate | No palate coverage |
| Taste sensation | Reduced (palate covered) | Improved | Full (no palate obstruction) |
| Speech impact | Lisp/click common | Minimal | None—closest to natural |
| Typical lifespan | 5–8 years | 15+ years (prosthesis), implants indefinite | 15–25 years (prosthesis), implants indefinite |
| Maintenance | Relining every 1–2 years, remake every 5–8 years | Attachment replacement every 1–2 years | Professional cleaning every 6 months |
| Approximate cost range | $1,000–$3,000 | $8,000–$15,000 | $15,000–$30,000 per arch |
The 20-Year Cost Analysis: Dentures vs. Implants
The upfront cost of implant treatment is higher, and that number causes sticker shock for many patients. But dentistry is a long-term investment, and the 20-year total cost tells a very different story than the day-one price tag.
Traditional dentures over 20 years:
- Initial denture: $2,000
- Relining (every 1–2 years × 10 relinings): $3,000–$5,000
- Replacement dentures (every 5–8 years × 3 remakes): $6,000–$9,000
- Adhesive costs ($20–$40/month × 240 months): $4,800–$9,600
- Bone grafting if implants are needed later (due to advanced resorption): $3,000–$8,000
- Total 20-year estimate: $15,800–$33,600
Implant overdentures over 20 years:
- Initial implants + overdenture: $10,000–$15,000
- Attachment replacements (every 1–2 years): $1,500–$3,000
- One prosthesis replacement at year 10–15: $3,000–$5,000
- Total 20-year estimate: $14,500–$23,000
Fixed full-arch bridge over 20 years:
- Initial All-on-4 treatment: $15,000–$30,000
- Professional cleanings and maintenance: $2,000–$4,000
- Possible prosthesis replacement at year 15–20: $5,000–$8,000
- Total 20-year estimate: $22,000–$42,000
The overdenture option is cost-competitive with traditional dentures over 20 years — and delivers dramatically better quality of life. The fixed bridge has a higher total cost but eliminates the daily hassle of removable prosthetics entirely.
These estimates do not factor in the indirect costs of denture limitations: the nutritional consequences of restricted diets, the social and professional costs of denture insecurity, or the potential medical costs associated with malnutrition in older adults. A 2020 study in the Journal of the American Geriatrics Society found that edentulous adults with poorly fitting dentures had a 21 percent higher risk of malnutrition compared to those with implant-supported restorations.
Quality of Life: What the Research Shows
The subjective experience of living with dentures versus implant-supported restorations is well documented in the clinical literature:
- A 2021 systematic review in the Journal of Dental Research analyzed 14 randomized controlled trials and found that patients with implant overdentures reported significantly higher satisfaction scores across all domains—comfort, stability, chewing ability, speech, and aesthetics—compared to conventional denture wearers.
- The Oral Health Impact Profile (OHIP-14), a standardized quality-of-life questionnaire, consistently shows that implant-supported prosthesis wearers score 40 to 60 percent better than conventional denture wearers, with the largest improvements in functional limitation and physical pain domains.
- A 2019 study in Clinical Oral Implants Research followed 120 patients for five years after All-on-4 treatment and reported that 97 percent said they would choose the same treatment again, and 94 percent rated their overall satisfaction as "excellent."
- Patients from Framingham, Sudbury, Westborough, and across MetroWest who have upgraded from dentures to implant-supported restorations at our office consistently describe the experience in the same terms: "I can eat again," "I stopped worrying about my teeth," "I look like myself again."
Snap-On Dentures: A Popular Middle Ground
Snap-on dentures (also called snap-in dentures or locator overdentures) have become one of the most requested options at our Marlborough office. They combine the affordability of dentures with the stability of implants. Two to four implants are placed in the jawbone, and the denture "snaps" onto them using small attachment housings.
Why patients choose snap-on dentures:
- Eliminates adhesives entirely, the snap connection holds the denture firmly in place
- Removable for cleaning, easier hygiene than a fixed bridge, which requires water flossers and threaders
- Lower cost than fixed All-on-4, typically $8,000 to $15,000 compared to $15,000–$30,000 for a fixed bridge
- Fewer implants required, as few as two implants can support a lower snap-on denture
- Preserves jawbone, the implants provide the stimulation needed to slow bone resorption
- Reversible upgrade path, if you start with a two-implant overdenture and later decide you want a fixed bridge, additional implants can be placed to support the conversion
Snap-on dentures are particularly popular among patients who want a significant upgrade from traditional dentures but prefer the ability to remove and clean their prosthesis at night. They are also a good option for patients with moderate bone loss who want to minimize the need for grafting. For patients with even less bone available, mini dental implants offer a narrower-diameter alternative that can stabilize a lower denture with minimal surgery.
Lifestyle Impact
The difference between dentures and implant-supported restorations extends well beyond the dental chair. Implant patients consistently report being able to eat foods they had given up—steak, apples, corn on the cob, nuts, crusty bread—speaking more clearly without worrying about denture movement, and feeling more confident in social and professional settings.
Taste and enjoyment of food: Upper dentures cover the palate, which contains thousands of taste buds and sensory receptors. Implant overdentures can be designed with a reduced palate or no palate coverage at all, and fixed bridges never cover the palate. Patients who transition from a full-palate denture to an implant-supported option frequently say food tastes better—because it literally does. They are accessing taste receptors that were previously blocked.
Speech clarity: Denture movement during speech causes clicking sounds, lisping, and whistling on certain consonants. Implant-supported prostheses eliminate this entirely. Patients who work in public-facing roles—teachers, salespeople, healthcare workers, attorneys—tell us the speech improvement alone justified the investment.
Facial appearance: Implants maintain jawbone volume, which preserves the structural support for the lips, cheeks, and chin. Without this support, the lower face collapses inward over time, creating the "denture face" appearance—sunken cheeks, thin lips, prominent chin, deepened facial folds. Implant-supported restorations prevent this progression and can even reverse early changes by restoring proper vertical dimension.
Who Is a Candidate for the Upgrade?
The American Academy of Implant Dentistry (AAID) notes that most denture wearers are candidates for implant-supported options, even those who have experienced significant bone loss. The key factors Dr. Fatima evaluates during a candidacy consultation:
Bone volume and density: 3D CBCT imaging at our office measures the exact height, width, and density of your remaining jawbone. Minimum bone requirements for implant placement are approximately 10 mm of height and 6 mm of width for standard implants. If your bone is below these thresholds, bone grafting can rebuild the site. The All-on-4 technique, with its angled posterior implants, can often bypass areas of bone loss entirely—one of its major advantages.
General health: Uncontrolled diabetes, active chemotherapy, high-dose bisphosphonate therapy, and heavy smoking (more than one pack per day) are relative contraindications that need to be discussed and potentially managed before implant placement. Well-controlled diabetics, former smokers, and patients who have completed cancer treatment are generally good candidates.
Bone grafting for severe resorption: If you have worn conventional dentures for 15 or more years and have significant bone loss, grafting procedures can rebuild the jaw. Options include:
- Ridge augmentation, adds bone width using grafting material and a collagen membrane
- Sinus lift, elevates the sinus floor and adds bone to the upper jaw posterior region
- Block grafts, transplants a block of bone from another area (chin, ramus) to the deficient site
- Zygomatic implants, extra-long implants that anchor into the cheekbone (zygoma) for patients with severe upper jaw bone loss, avoiding grafting entirely
Realistic expectations: Implant treatment is a process, not an event. The timeline from initial consultation to final prosthesis delivery is typically 4 to 8 months, depending on whether grafting is needed. Patients who understand and commit to the timeline get the best results.
Caring for Implant-Supported Restorations
Implant-supported dentures and bridges require daily maintenance to ensure long-term success. The implants themselves are not susceptible to cavities, but the gum tissue and bone around them can develop peri-implantitis—an inflammatory condition similar to gum disease—if bacteria are allowed to accumulate.
For removable overdentures:
- Remove the prosthesis each night
- Clean the attachment housings with a soft brush
- Soak the denture in a cleaning solution (Efferdent, Polident, or a dilute chlorhexidine solution)
- Brush the implant abutments and surrounding gum tissue with a soft brush
- Rinse and reinsert in the morning
For fixed full-arch bridges:
- Use a water flosser (Waterpik) to flush debris from under the prosthesis and around the implant posts
- Use specialized floss threaders (Superfloss or implant-specific floss) to clean under the bridge at least once daily
- Brush the prosthesis surfaces with a soft brush and non-abrasive toothpaste
- Attend professional cleanings every 4 to 6 months—Dr. Fatima or our hygienist will remove the prosthesis periodically (typically once per year) for a deep cleaning of the implant components
Regular dental checkups, typically every six months, allow Dr. Fatima to inspect the implant sites, clean areas that are difficult to reach at home, and evaluate the condition of the prosthesis. With proper long-term care, implant-supported restorations provide decades of reliable function. A 2022 longitudinal study in the Clinical Oral Implants Research journal reported that implant overdentures maintained 94 percent implant survival at 20 years when patients followed recommended maintenance protocols.
E-E-A-T: Full-arch planning requires advanced surgical and prosthetic training. Dr. Fatima’s FICOI (Fellow of the International Congress of Oral Implantologists) and FAAIP (Fellow of the American Academy of Implant Prosthodontics) credentials represent hundreds of hours of advanced implant training and documented case experience. These fellowships go well beyond the implant education provided in general dental school.
Patients from Hudson, Hopkinton, Ashland, and across MetroWest
We see patients from every MetroWest community for implant consultations. Many have worn conventional dentures for years and assumed implants were not an option for them—either because of bone loss, age, or cost concerns. In the vast majority of cases, at least one implant-supported option is feasible, and our team works with you to find the solution that matches your anatomy, lifestyle, and financial situation.
If you are considering the transition from dentures to implants, the first step is a consultation that includes 3D CBCT imaging. This scan takes about 15 seconds and gives Dr. Fatima a complete picture of your bone anatomy. From there, she can present your specific options with honest timelines and cost estimates.
Ready to stabilize your smile? Call (508) 481-0110 or request a consultation.
Related Articles
- How Much Do Dentures Cost? Full & Partial Prices
- Snap-On Dentures: Cost, Benefits & How They Work
- All-on-4 Dental Implants: Full Mouth Restoration Guide
- The Real Cost of Dental Implants in Massachusetts